A Clinical Pilates Perspective
Cervical disc disease, whether due to degenerative disc changes, disc bulging, or herniation, is a common source of neck pain, radicular symptoms, and movement dysfunction in Pilates clients. As an instructor, understanding the underlying pathomechanics and appropriate exercise selection is essential for promoting both safety and therapeutic benefit.
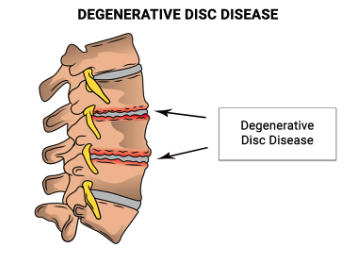
Understanding The Condition
Cervical disc disease involves structural degeneration or displacement of the intervertebral disc, often most pronounced at the C5–C6 and C6–C7 levels. This may lead to nerve root irritation, reduced cervical stability, and compensatory overactivity of superficial neck musculature. Clients frequently present with neck stiffness, radiating arm symptoms, or postural dysfunction (e.g., forward head and rounded shoulder posture).
The clinical goal in a Pilates setting is to reduce compressive load, enhance deep cervical stabilizer activation, and restore balanced movement control through the cervical and shoulder girdle complex.
Adjunct Technique: Cervical Traction
Cervical traction can be a beneficial adjunct for clients with disc pathology, as it helps decompress the intervertebral spaces, reduce radicular pain, and decrease neural tension. Gentle manual or mechanical traction—when medically approved—can relieve symptoms and prepare the client for exercise by improving alignment and decreasing muscle guarding.
In a Pilates context, this concept translates to maintaining axial elongation and spinal decompression cues throughout movement. Encourage clients to “lengthen the back of the neck” and “float the head away from the shoulders” to create a self-traction effect during exercises.
Indicated Pilates Exercises
Created with