The shoulder is composed of several articulations, but the two most functionally significant in arm elevation are:
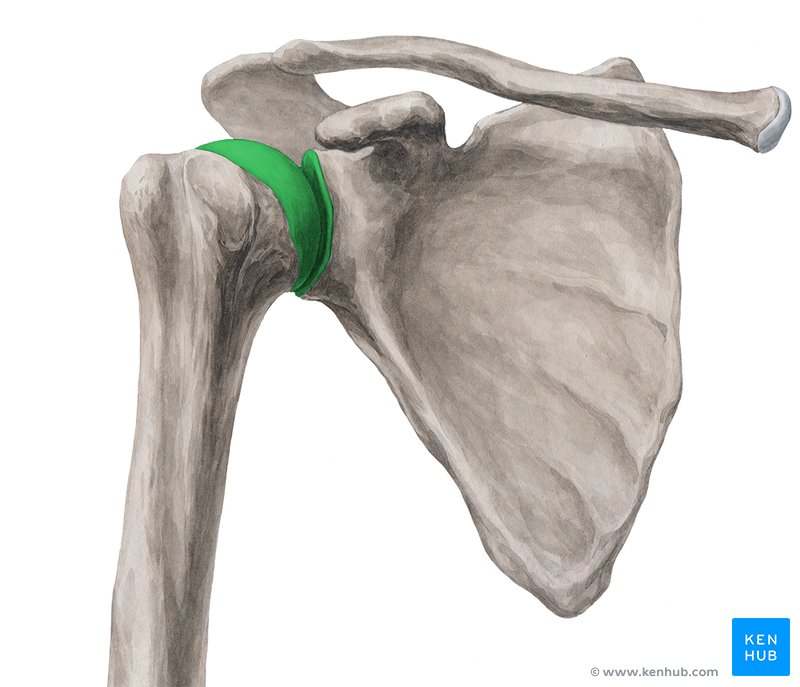
Glenohumeral (GH) Joint
A synovial ball-and-socket joint formed by the articulation of the large humeral head and the shallow glenoid fossa of the scapula, which allows for movement in multiple planes:
- Flexion / Extension
- Abduction / Adduction
- Horizontal abduction / Adduction
- Internal / External Rotation
Scapulothoracic (ST) Articulation
Not a true synovial joint, but a functional articulation between the scapula and thoracic rib cage controlled entirely by muscular activity and enables:
- Elevation / Depression
- Protraction / Retraction
- Upward / Downward Rotation
Together, these joints function in synchrony to enable overhead motion and shoulder stability.
When the arm moves into flexion or abduction beyond ~60 degrees, the glenohumeral joint can no longer function independently. To continue upward motion without causing impingement between the humeral head and the acromion, the scapula must rotate upward and reposition on the thorax.
This coordination between the humerus and the scapula follows a predictable pattern known as the scapulohumeral rhythm.
For every 3 degrees of shoulder elevation:- 2 degrees occur at the glenohumeral joint
- 1 degree occurs at the scapulothoracic articulation
In other words, the humerus moves twice as fast as the scapula. This ratio ensures that the shoulder complex moves efficiently while preserving joint space and minimizing mechanical stress.
Proper scapulohumeral rhythm depends on a balance of muscular force couples, which stabilize and guide joint motion during elevation:
Deltoid and Rotator Cuff:
- The deltoid initiates elevation, pulling the humerus upward.
- The rotator cuff (especially the infraspinatus, subscapularis, and teres minor) provides a downward and compressive force, centering the humeral head in the glenoid to prevent superior migration.
Trapezius and Serratus Anterior:
- The upper trapezius, lower trapezius, and serratus anterior work together to produce upward rotation of the scapula.
- The serratus anterior, in particular, stabilizes the scapula against the thoracic wall and prevents winging during arm elevation.
When scapulohumeral rhythm is altered, either due to weakness, stiffness, poor motor control, or pain, it can result in inefficient or pathological movement patterns that increase the risk of injury. Common dysfunctions include:

1. Subacromial Impingement Syndrome (SAIS): Inadequate upward rotation or posterior tilt of the scapula reduces the subacromial space, compressing the supraspinatus tendon, bursa, or long head of the biceps tendon.
2. Rotator Cuff Pathology: When the deltoid overpowers a weak or inhibited rotator cuff, the humeral head migrates superiorly, contributing to tendinopathy or partial/full thickness tears over time.
3. Scapular Dyskinesis: Abnormal scapular positioning or movement, often seen in overhead athletes or individuals with postural deficits, disrupts normal rhythm and affects performance and endurance.
4. Adhesive Capsulitis (Frozen Shoulder): Limited GH mobility results in compensatory scapular motion, often exaggerating scapulothoracic contribution and altering the typical 2:1 rhythm.
As movement practitioners, observing arm elevation must go beyond GH range of motion. Assessment of scapular motion, timing, and muscle activation is essential.
What to Look for in Your Pilates Sessions- Watch how the scapula moves during shoulder lifts, especially in flexion and abduction.
- Look for smooth, controlled upward rotation and timing with the arm.
- Notice any signs of compensation, like shoulder hiking, winging, or delayed scapular movement.
- Use tactile cueing to help clients find better scapular placement and control during arm work.
- Observe how posture affects movement, especially in exercises like arm circles, rowing, or overhead press work.

- Focus on coordination and timing. Use slow, mindful movement to retrain proper sequencing between the arm and shoulder blade.
- Strengthen key stabilizers, such as the serratus anterior and lower trapezius, using exercises like wall slides, arm arcs with scapulare awareness, and swan variations with shoulder blade focus.
- Open the front of the body. Stretch tight areas like the chest (pectoralis minor) with movements that promote thoracic extension and scapular retraction (e.g., breaststroke prep, chest expansion).
- Emphasize alignment and breath to support optimal motor control and reduce compensation patterns.
The scapulohumeral rhythm is not just a theoretical ratio; it's a clinical cornerstone for healthy shoulder function. An efficient, coordinated movement between the scapula and humerus allows patients to perform daily and athletic activities pain-free and with longevity. For rehabilitation professionals, recognizing early signs of rhythm dysfunction can help prevent chronic pathology and optimize shoulder recovery. injuries require a thoughtful, phase-based approach to exercise. With a deep understanding of knee biomechanics and healing timelines, Pilates-based rehabilitation offers a safe and effective way to regain mobility, build strength, and reduce the risk of re-injury.
For professionals working with clients recovering from meniscus tears, knowing which movements to emphasize and which to modify is essential. With careful observation and purposeful cueing, Pilates can support long-term joint health and functional recovery.